Total hip replacement is one of the most successful treatment
interventions in current medical practice. In this operation, the
ball and socket of the natural hip joint are replaced by a
prosthetic joint.
A large number of people have hip replacements and this page is
intended to help the reader understand hip replacement operations,
their advantages and disadvantages, and the
limitations.
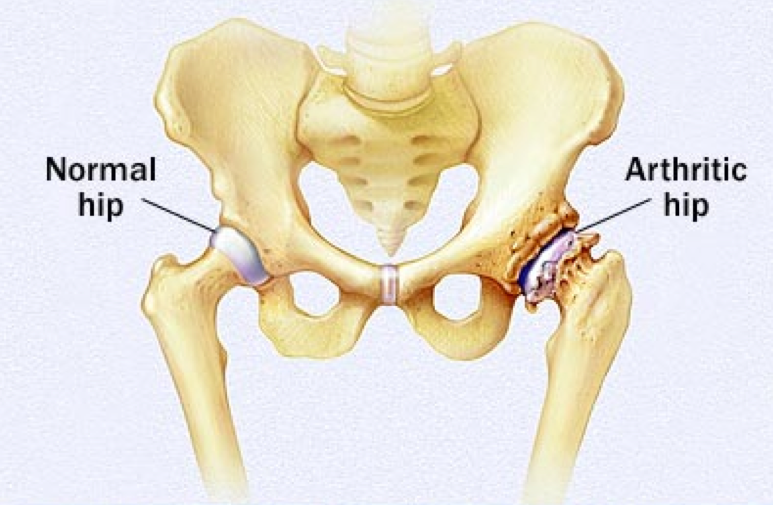
Arthritis of the
hip
The natural hip joint has a socket called the
acetabulum, which is a part of the pelvic bone. The top end of the
thigh bone, called the head of femur, is rounded and fits into the
socket to form the hip joint. The articulating surface of the
acetabulum and head of femur is lined with a very smooth covering
called the articular cartilage.
In arthritis, the articular cartilage becomes thin and wears out.
Various conditions can affect the integrity of the articular
cartilage. Most commonly, it is osteoarthritis (also called as
osteoarthrosis), and other conditions include rheumatoid arthritis,
arthritis following injury to the hip, ankylosing spondylitis,
arthritis secondary to malformation of the hip, gout, Paget’s
disease, and rarely tumours and infections.
Hip replacement is carried out to relieve pain from the degenerate
joint.